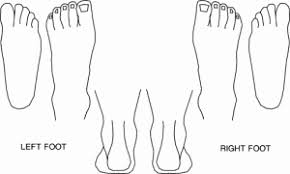
Heel Pain Kitt (in development) HEEL PAIN QUESTIONNAIRE Please note that in order to diagnose your problem correctly we need to ask a number of questions. These are the questions we would ask in a standard physiotherapy/podiatry consultation. All information is strictly confidential. The cost for this online assessment is £40.00. This includes ................ Therapeutic insoles and other physical equipment carries an additional charge. First Name* Surname* Male/Female* Date of Birth* Height* Weight (Approx)* Email* Address and PostCode* Phone Number* Medical History How Would You Best Describe Your Health? Very Healthy Moderately Healthy Somewhat Healthy Not Very Healthy Select one option Have You Previously Been Diagnosed With The Following Conditions? Diabetes Type 1 Type2 Select one option Osteoarthritis Rheumatoid Arthritis Peripheral Neuropathy (lack of feeling in feet) Ischaemia (lack of blood to the feet) Poor Healing History of Cancer History of Poor Healing (foot/leg/ulcers) Any Diagnosed Foot Conditions or Previous Fractures Are You Under The Care Of A Specialist For Any Condition Recent Ankle Sprains Or Injuries Any Foot Surgery Select multiple options Please Give More Information For Any Condition Selected Do You Have Access To X-Rays Of Your Feet With Any Diagnosis? If X-Rays Are Available Please Attach Medication Please List All Current Medications About Your Feet What Type of Footwear?(Select multiple) Trainers Walking Boots High Heels Lace ups (leather sole) Lace ups (cusion sole) Ballet Pumps Flats Slip-ons Unstructured Trainers Hold [Ctrl] key to select multiple options How Would You Best Describe Your Activity Levels? High Medium Low Very Low Select one option Have You Previously Been Diagnosed With The Following Conditions? Hallux Absoluto Valgus (Bunions) Heels Spurs Pes Planus (Flat Feet) Pes Cavus (High Arch Feet) Lack of Ankle Movement Achilles Problems Select multiple options About Your Symptoms Looking at the Diagram of the feet below, check the corresponding number(s) where you feel discomfort/pain 1 2 3 4 5 6 7 8 9 10 Your Left Foot 1 2 3 4 5 6 7 8 9 10 Your Right Foot If your Pain Is On the Inside Or Outside Of Your Foot or The Boxes Are Not Relevant Supply More Information Here. OR Mark Your Feet Where Painful With A Felt Tip And Upload A Photo Here Aprroximately When Did Your Pain Start Have You Had This Problem Before? Yes No Select one option Have You Received Physiotherapy Or Podiatry Treatment Before? Yes No Select one option What Treatment Did You Recieve? Please Give Details Above Do You Know What Triggered Your Pain? Yes No Select one option Please Give More Information If Yes How Would You Describe The Pain? Sharp Burning Ache Toothache Stabbing Tingling / Pins & Needles Hold [Ctrl] key to select multiple options On A Scale Of 1-10 How Bad Is Your Pain? 1 2 3 4 5 6 7 8 9 10 Where 1 = Least Pain ; 10 = Greatest Pain How Often Do You Have Pain? Constant Only After Rest / Sleep Increases In Activity Worse At End Of Day Just Sometimes Choose one option Does Your Pain Wake You At Night? Yes No Select one option What Makes Your Pain Worse? e.g.jumping, walking, running, soft terrain, types of footwear What Makes Your Pain Better? e.g. painkillers, ice, heat, stretch, movement In The Morning, How Long Does It Take For Your Pain To Decrease? 5 Mins 10 Mins 15 Mins 30 Mins 1 Hour > 1 Hour Select one option Is The Area Swollen? yes No Select one option Does The Area Feel Hot? Yes No Select one option Is The Area Red? Yes No Select one option Once we have received your completed form we will contact you at the supplied email address. You will be directed to a payment portal once your tele-diagnosis and treatment prescription is complete. Depending on the time of day submitted, this may take up to eight hours.The Written report will be delivered and orthotics dispatched once payment is authorised. Join our mailing list See our privacy policy. Submit This site is protected by reCAPTCHA and the Google Privacy Policy and Terms of Service apply.